What is Diastasis Recti?
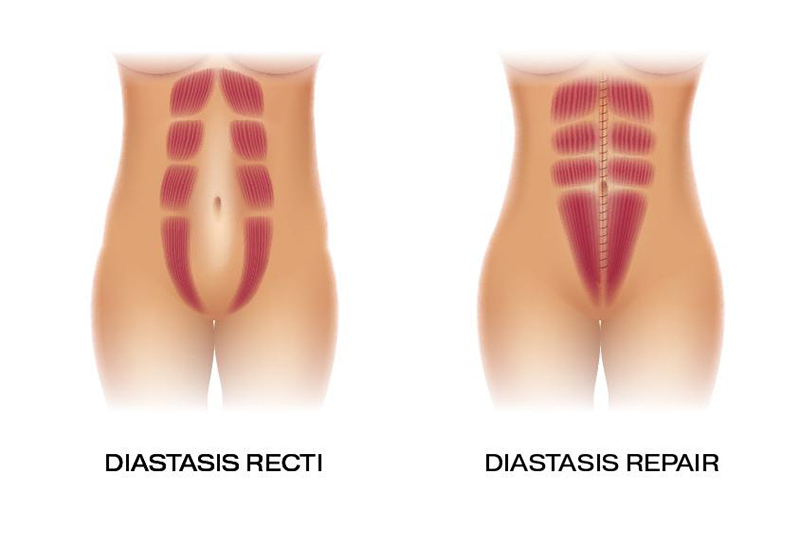
Diastasis recti is the separation of the two rectus abdominis muscles along the linea alba — the fibrous connective tissue that runs vertically down the midline of your abdomen. When intra-abdominal pressure exceeds what this tissue can withstand, the linea alba stretches and thins, causing the muscle columns to drift apart. A gap of more than 2.5 cm is considered clinically significant and is unlikely to resolve without treatment.
In Manchester & Cheshire, Mr Nassab sees diastasis recti most commonly in postpartum women, but it can also affect men, infants, and non-pregnant women — particularly those who have experienced rapid weight change or performed high-load abdominal training with poor technique.